As you scroll through this timeline, you will learn about some of the key milestones in the history and
evolution of our understanding in Duchenne muscular dystrophy (DMD). We begin with the initial description
of DMD in 1861 and follow the evolution of the care and management of people living with DMD through to
today. Let's take a look.
How to use the timeline
Click & drag to move along timelineScroll to move down timeline
Click for
referencesPress for references
Click for more informationPress for more information
Click for information on patientsPress for information on patients
1861
DMD description
The French neurologist Guillaume-Benjamin-Amand Duchenne accurately describes in great detail a case of
DMD in a young boy with a progressive muscle disease and significant physical-motor impairment linked to
muscle hypertrophy in his book.
References
Parent A. Duchenne De Boulogne: a pioneer in neurology and medical photography. Can J Neurol Sci.
2005;32(3):369-377.
DMD description
The disorder that would eventually be called Duchenne muscular dystrophy was actually first
described nearly 30 years earlier by two Italian physicians (Giovanni Semmola in 1834 and Gaetano
Conte in 1836). Nonetheless, Duchenne describes and details the case of a boy who had this
condition in the 1861 edition of his book
Paraplegie hypertrophique de l'enfance de cause cerebrale, and he will present photos of
his patient in his Album de photographies pathologiques a year later.
References
Bissonnette B, Luginbuehl I, Engelhardt T. Duchenne muscular dystrophy. In:
Syndromes: Rapid Recognition and Perioperative Implications. 2nd ed. McGraw-Hill
Education; 2019.
https://accessanesthesiology.mhmedical.com/content.aspx?bookid=2674§ionid=220528088.
Accessed April 20, 2020.
Motor skill decline to non-ambulatory at 10 years of age
Outcome
Died at 18 years of age due to respiratory infections and cardiomyopathy
References
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy:
report from International Working Group meetings.
Clin Investig (Lond). 2011;1(9):1217-1235.
Ciafaloni E, Fox DJ, Pandya S, et al. Delayed diagnosis in Duchenne muscular dystrophy: data
from the muscular dystrophy surveillance, tracking, and research network (MD STARnet).
J Pediatr. 2009;155(3):380-385
Gardner-Medwin. Duchenne muscular dystrophy: early diagnosis, and screening.
Arch Dis Child. 1976;51(1):982-983.
Corticosteroid use
The first clinical trial evaluating the safety and efficacy of a corticosteroid (prednisone) in DMD is
published, setting the stage for a potential palliative treatment option for some patients.
References
Drachman DB, Toyka KV, Myer E. Prednisone in Duchenne muscular dystrophy. Lancet. 1974;2(7894):
1409-1412.
1987
DMD cloning
American geneticist Louis M. Kunkel’s group clones the DMD cDNA, enabling him and others to begin to
identify mutations from patients with DMD.
References
Koenig M, Hoffman EP, Bertelson CJ, et al. Complete cloning of the Duchenne muscular dystrophy (DMD)
cDNA and preliminary genomic organization of the DMD gene in normal and affected individuals.
Cell. 1987;50(3):509-517.
Dystrophin description
Shortly after cloning the DMD gene, Dr Kunkel’s group describes the gene’s protein product, which they
name dystrophin. This leads to the landmark discovery that boys with DMD lack dystrophin.
References
Hoffman EP, Brown RH Jr, Kunkel LM. Dystrophin: the protein product of the Duchenne muscular
dystrophy locus. Cell. 1987;51(6):919-928.
1988
Dystrophin for DMD diagnosis
The discoveries by Kunkel and others lead to the use of muscle biopsies to characterize dystrophin
levels and thereby diagnose patients with DMD.
References
Hoffman EP, Fischbeck KH, Brown RH, et al. Characterization of dystrophin in muscle-biopsy specimens
from patients with Duchenne’s or Becker’s muscular dystrophy.
N Engl J Med. 1988;318(21):1363-1368.
1990
DMD deletions for diagnosis
Advances in polymerase chain reaction (PCR) technology result in diagnostic tests that can detect 98% of
deletions in DMD through blood samples.
References
Beggs AH, Koenig M, Boyce FM, et al. Detection of 98% of DMD/BMD gene deletions by polymerase chain
reaction. Hum Genet. 1990;86(1):45-48.
DMD deletions for diagnosis
During the late 1980s and early 1990s, diagnosis of DMD typically requires a muscle biopsy. This
biopsy is used to evaluate dystrophin protein expression. With the progress made in technology enabling the analysis of DNA, the recommended stepwise process for diagnosis of DMD was muscle biopsy, PCR, and then Southern Blotting. PCR and Southern blotting enabled evaluation of molecular
changes in the DMD gene. Furthermore, with the continuing development of assays to detect genetic
mutations from peripheral blood, the hope is that diagnosis of DMD would be performed by PCR without
the need for muscle biopsy.
References
Beggs AH, Koenig M, Boyce FM, et al. Detection of 98% of DMD/BMD gene deletions by polymerase
chain reaction. Hum Genet. 1990;86(1):45-48.
Corticosteroids are studied to evaluate efficacy and safety in patients with DMD.
References
Griggs RC, Moxley RT 3rd, Mendell JR, et al. Prednisone in Duchenne dystrophy. A randomized, controlled trial defining the time course and dose response. Clinical Investigation of Duchenne Dystrophy Group. Arch Neurol. 1991;48(4):383-388.
Mendell JR, Moxley RT, Griggs RC, et al. Randomized, double-blind six-month trial of prednisone in Duchenne's muscular dystrophy. N Engl Med. 1989;320(24):1592-1597.
Mesa LE, Dubrovsky AL, Corderi J, et al. Steroids in Duchenne muscular dystrophy--deflazacort trial. Neuromuscul Disord. 1991;1(4):261-266.
1992
Nonsense mutations in DMD
David Bentley’s group identifies nonsense mutations in the dystrophin gene of 4 out of 7 patients with
DMD or intermediate muscular dystrophy, in whom no deletion was detected by multiple PCR. A nonsense
mutation is a point mutation that changes a codon into an in-frame premature stop codon, resulting in
premature termination of dystrophin translation and disease pathogenesis.
References
Roberts RG, Bobrow M, Bentley DR. Points mutations in the dystrophin gene.
Proc Natl Acad Sci U S A. 1992; 89(6):2331-2335.
Nonsense mutations in DMD
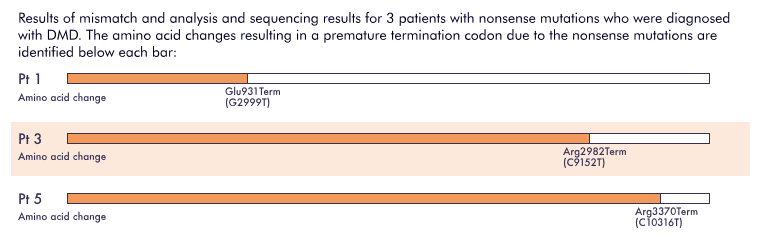
The diagram below highlights mutations identified in the dystrophin gene in 3 of 4 these patients
with nonsense mutations. The results of these analyses suggest that truncation of the dystrophin
protein negatively impacts its function and contributes to disease pathogenesis. Since this
discovery, over 4700 mutations have been linked to DMD, with roughly 10% to 15% making up small
nonsense mutations in the DMD gene (nmDMD).
References
Pichavant C, Aartsma-Rus A, Clemens PR, et al. Current status of pharmaceutical and genetic
therapeutic approaches to treat DMD. Mol Ther. 2011;19(5):830-840.
Roberts RG, Bobrow M, Bentley DR. Points mutations in the dystrophin gene.
Proc Natl Acad Sci U S A. 1992; 89(6):2331-2335.
Winnard AV, Jia-Hsu Y, Gibbs RA, et al. Identification of a 2 base pair nonsense mutation
causing a cryptic splice site in a DMD patient. Hum Mol Genet. 1992;1(8):645-646.
Name: Benjamin
Signs and symptoms at diagnosis
Muscle weakness with Gower’s maneuver, family history (a brother with DMD)
Age at diagnosis
5 years
Diagnostic method
Muscle biopsy followed by molecular testing
(Southern blotting) for dystrophin
Management/treatment options
Oral daily prednisone
Progression
Becomes non-ambulatory at 10 years of age and receives spinal surgery for scoliosis at 14 years of
age
Outcome
Died at 21 years of age due to cardiac and respiratory complications
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy:
report from International Working Group meetings.
Clin Investig (Lond). 2011;1(9):1217-1235.
Bushby K, Finkel R, Birnkrant DJ, et al; DMD Care Considerations Working Group. Diagnosis
and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and
psychosocial management. Lancet Neurol. 2010;9(1):77-93.
DeSilva S, Drachman DB, Mellits D, et al. Prednisone treatment in Duchenne muscular
dystrophy.
Arch Neurol. 1987;44(8):818-822.
Finder JD, Birnkrant D, Carl J, et al; American Thoracic Society. Respiratory care of the
patient with Duchenne muscular dystrophy: ATS consensus statement.
Am J Respir Crit Care Med. 2004;170(4):456-465.
Pandya S, James KA, Westfield C, et al. Health profile of a cohort of adults with Duchenne
muscular dystrophy. Muscle Nerve. 2018;58(2):219-223.
1998
Founding of PTC Therapeutics
Under the leadership of Dr Stuart Peltz, PTC Therapeutics is founded in New Jersey, USA. The PTC
readthrough program is initiated to help identify small molecules that can read through nonsense
mutations.
This point denotes when PTC Therapeutics was founded based on their readthrough program. We will begin
exploring the process of rare disease drug development through this
lowerleft hand timeline.
Swipe to switch between the two timeline views
2004
Respiratory care guidelines
As respiratory disease in DMD is a major cause of morbidity and mortality, the American Thoracic
Society (ATS) creates respiratory care guidelines for patients with DMD, highlighting:
Evaluation and anticipatory guidance for patients with DMD
Management options for respiratory complications related to DMD
References
Finder JD, Birnkrant D, Carl J, et al; American Thoracic Society. Respiratory care of the patient
with Duchenne muscular dystrophy: ATS consensus statement.
Am J Respir Crit Care Med. 2004;170(4):456-465.
2005
Corticosteroid use
The American Academy of Neurology (AAN) develops the first practice parameter document recommending
the use of corticosteroids in patients with DMD.
References
Moxley RT III, Ashwal S, Pandya S, et al; Quality Standards Subcommittee of the American Academy
of Neurology; Practice Committee of the Child Neurology Society. Practice parameter:
corticosteroid treatment of Duchenne dystrophy: report of the Quality Standards Subcommittee of
the American Academy of Neurology and the Practice Committee of the Child Neurology Society.
Neurology. 2005;64(1):13-20.
Genetics for DMD diagnosis
Genetic analysis techniques continue to evolve and can detect most mutations in patients with a
clinical diagnosis of muscular dystrophy (e.g., DMD or Becker muscular dystrophy).
References
Flanigan KM, von Niederhausern A, Dunn DM, et al. Rapid direct sequence analysis of the dystrophin
gene.
Am J Hum Genet. 2003;72(4):931-939.
Gatta V, Scarciolla O, Gaspari AR, et al. Identification of deletions and duplications of the DMD
gene in affected males and carrier females by multiple ligation probe amplification (MLPA).
Hum Genet. 2005;117(1):92-98.
2007
Life expectancy
With the current standard of care, the average life expectancy for patients is in the third decade of
life.
References
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy: report
from International Working Group meetings. Clin Investig (Lond). 2011;1(9):1217-1235.
Nonsense readthrough agent
Identification of a nonsense readthrough agent that may have broad clinical potential for
certain genetic diseases is published in Nature.
References
Welch EM, Barton ER, Zhuo J, et al. PTC124 targets genetic disorders caused by nonsense mutations.
Nature. 2007;447(7140):87-91.
2007
Nonsense readthrough agent
Identification of a nonsense readthrough agent that may have broad clinical potential for
certain genetic diseases is published in Nature.
References
Welch EM, Barton ER, Zhuo J, et al. PTC124 targets genetic disorders caused by nonsense mutations.
Nature. 2007;447(7140):87-91.
2010
DMD guidelines
Comprehensive, international guidance for the diagnosis and management of patients with DMD is
developed. This guidance aims to:
Raise awareness of DMD
Help improve the quality and standardization of care for patients with DMD
References
Ward LM, Birnkrant DJ. An introduction to the Duchenne muscular dystrophy care considerations.
Pediatrics. 2018;142(suppl 2):S1-S4.
Name: Eric
Signs and symptoms at diagnosis
Muscle weakness, Gower’s maneuver, differences in motor skills compared with peers, elevated
serum creatine kinase
Age at diagnosis
5 years
Diagnostic method
Multiplex PCR for DMD mutation, which identified a deletion in DMD
Management/treatment options
Prednisone and physical therapy
Progression
Becomes non-ambulatory at 13 years of age; no surgery needed for scoliosis
Outcome
Died at 29 years of age due to cardiac and respiratory complications
References
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy:
report from International Working Group meetings.
Clin Investig (Lond). 2011;1(9):1217-1235.
Bushby K, Finkel R, Birnkrant DJ, et al; DMD Care Considerations Working Group. Diagnosis
and management of Duchenne muscular dystrophy, part 1: diagnosis, and pharmacological and
psychosocial management. Lancet Neurol. 2010;9(1):77-93.
Ciafaloni E, Fox DJ, Pandya S, et al. Delayed diagnosis in Duchenne muscular dystrophy:
data from the muscular dystrophy surveillance, tracking, and research network (MD
STARnet).
J Pediatr. 2009;155(3):380-385.
Henricson EK, Abresch RT, Cnaan A, et al.; CINRG Investigators. The cooperative
international neuromuscular research group Duchenne natural history study: glucocorticoid
treatment preserves clinically meaningful functional milestones and reduces rate of
disease progression as measured by manual muscle testing and other commonly used clinical
trial outcome measures. Muscle Nerve. 2013;48(1):55-67.
Pandya S, James KA, Westfield C, et al. Health profile of a cohort of adults with Duchenne
muscular dystrophy. Muscle Nerve. 2018;58(2):219-223.
2011
Developing therapies for DMD
A review article highlights potential therapeutic options in development for DMD, including a nonsense
readthrough agent and antisense oligonucleotides that aims to increase endogenous dystrophin
production.
References
Pichavant C, Aartsma-Rus A, Clemens PR, et al. Current status of pharmaceutical and genetic
therapeutic approaches to treat DMD. Mol Ther. 2011;19(5):830-840.
2011
Natural history of DMD
On behalf of the International Working Group on DMD clinical outcomes, Dr Kate Bushby and Dr Edward
Connor summarize discussions from a workshop, including a description of the natural history of DMD in
the era of corticosteroids. This information and that of clinical trial control data sets are integral
to help develop better end points for future clinical trials of investigative therapies for DMD.
References
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy: report
from International Working Group meetings. Clin Investig (Lond). 2011;1(9):1217-1235.
Natural history of DMD
Natural history studies for rare diseases are crucial to pave the way for improved disease
understanding and better clinical trial end points. In addition, some of the natural history
studies in DMD helped identify optimal baseline characteristics of patients for clinical trial
enrollment using
Longitudinal observations of motor function
Longitudinal, multicenter, clinical history of patients with DMD
Over time, these studies also included characteristics of patients who received corticosteroids.
References
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy:
report from International Working Group meetings.
Clin Investig (Lond). 2011;1(9):1217-1235.
Humbertclaude V, Hamroun D, Bezzou K, et al. Motor and respiratory heterogeneity in Duchenne
patients: implication for clinical trials.
Eur J Paediatr Neurol. 2012;16(2):149-160.
Mazzone E, Vasco G, Sormani MP, et al. Functional changes in Duchenne muscular dystrophy: a
12-month longitudinal cohort study. Neurology. 2011;77(3):250-256.
2013
2013
Natural history of DMD
Several research groups publish natural history studies of patients with DMD to better understand the
disease progression and to help improve clinical trial end points.
References
Bushby K, Finkel R, Wong B, et al; PTC124-GD-007-DMD Study Group. Ataluren treatment of patients
with nonsense mutation dystrophinopathy.
Muscle Nerve. 2014;50(4):477-487.
McDonald CM, Henricson EK, Abresch RT, et al. The 6-minute walk test and other endpoints in
Duchenne muscular dystrophy: longitudinal natural history observations over 48 weeks from a
multicenter study. Muscle Nerve. 2013;48(3):343-356.
Natural history of DMD
With the natural history studies that have been published, many factors have been investigated as
potential end points for ambulatory DMD trials. Some of these end points include time to
persistent 10% 6MWD worsening and the 6MWD test. Notably, baseline 6MWD has prognostic value, both
for primary assessment of walking and secondary assessments of function, muscle strength,
activity, and fall frequency. The results of these studies support a clinically meaningful change
in 6MWD to be approximately 20 to 30 meters, which can be a target treatment effect among
ambulatory patients with DMD.
References
Bushby K, Finkel R, Wong B, et al; PTC124-GD-007-DMD Study Group. Ataluren treatment of
patients with nonsense mutation dystrophinopathy.
Muscle Nerve. 2014;50(4):477-487. McDonald CM, Henricson EK, Abresch RT, et al. The
6-minute walk test and other endpoints in Duchenne muscular dystrophy: longitudinal natural
history observations over 48 weeks from a multicenter study.
Muscle Nerve. 2013;48(3):343-356.
2015
CK-M in DMD
The discovery of elevated serum muscle-type creatine kinase (CK-M) in patients with DMD provides an
opportunity for the use of a non-invasive biomarker to help monitor disease progression.
References
Burch PM, Pogoryelova O, Goldstein R, et al. Muscle-derived proteins as serum biomarkers for
monitoring disease progression in three forms of muscular dystrophy.
J Neuromuscul Dis. 2015;2(3):241-255.
Dystrophin mutations in DMD
With advances in disease understanding, genotype-phenotype correlations in muscular dystrophy are
identified, which have implications for diagnosis, prediction of prognosis, and management. Different
procedures and tools to identify these mutations become integral to the diagnosis of DMD and other
dystrophies.
References
Falzarano MS, Scotton C, Passarelli C, et al. Duchenne muscular dystrophy: from diagnosis to
therapy. Molecules. 2015;20(10):1816&zwj8-18184.
Dystrophin mutations in DMD
Amino acids, the building blocks of protein, are coded for by 3 nucleotide sequences in a gene. When a mutation is found within the gene sequence, it may lead to changes in the translated protein. For example, section B of the diagram shows how the deletion of exons 47-50 in the dystrophin gene shifts the nucleotide reading frame. This frameshift results in an incorrect sequence of amino acids being incorporated after the deletion during translation, leading to a non-functional protein and DMD. In contrast, section C of the diagram shows how the deletion of exons 46-54 in the dystrophin gene maintains the reading frame. The gene is transcribed and translated to produce a truncated but partially functional dystrophin protein, leading to Becker muscular dystrophy (BMD). Note that there are exceptions to this rule that mutations that disrupt the reading frame lead to DMD and mutations that maintain the reading frame lead to BMD.
The molecular tools to help diagnose DMD include
Multiplex ligation-dependent probe amplification, microarray-based comparative genomic
hybridization, and next-generation sequencing to identify deletion/duplication of exons
Microarray-based comparative genomic hybridization, reverse transcription PCR, and fluidic
card to identify complex mutations
Sanger sequencing and next-generation sequencing to identify point mutations, including
nonsense mutations
References
Aartsma-Rus A, Ginjaar IB, Bushby K. The importance of genetic diagnosis for Duchenne
muscular dystrophy. J Med Genet. 2016;53(3):145-151.
Berg JM, Tymoczko JL, Stryer L. Section 5.5 Amino acids are encoded by groups of three bases
starting from a fixed point. Biochemistry. 5th edition. New York: W H Freeman;
2002.
Falzarano MS, Scotton C, Passarelli C, et al. Duchenne muscular dystrophy: from diagnosis to
therapy. Molecules. 2015;20(10):181&zwj68-18184.
Pichavant C, Aartsma-Rus A, Clemens PR, et al. Current status of pharmaceutical and genetic
therapeutic approaches to treat DMD. Mol Ther. 2011;19(5):830-840.
Wang L, Xu M, Li H, et al. Genotypes and phenotypes of DMD small mutations in Chinese
patients with dystrophinopathies. Front Genet. 2019;10:114.
STRIVE award
The Strategies to Realize Innovation, Vision and Empowerment (STRIVE) award is presented for the first
time. The award provides grants to different organizations in recognition of their efforts to meet the
needs of the Duchenne community around the world.
The North Star Ambulatory Assessment (NSAA) is revised to be suitable for boys with DMD between the
ages of 3 and 5 years, forming an age-appropriate outcome measure for these patients.
References
Mercuri E, Coratti G, Messina S, et al. Revised North Star Ambulatory Assessment for young boys
with Duchenne muscular dystrophy. PLoS One. 2016;11(8):e0160195. doi:
10.1371/journal.pone.0160195.
Updated corticosteroid guidelines
About a decade after the first corticosteroid treatment guidelines are published, AAN updates their
practice guidelines to address several key points:
Efficacy of corticosteroids for survival, quality of life, motor function, scoliosis, pulmonary
function, and cardiac function
Comparison of prednisone and deflazacort
Adverse events associated with corticosteroids
Interventions to maximize bone health
References
Gloss D, Moxley RT 3rd, Ashwal S, et al. Practice guideline update summary: Corticosteroid
treatment of Duchenne muscular dystrophy: Report of the Guideline Development Subcommittee of the
American Academy of Neurology. Neurology. 2016;86(5):465-472.
Updated corticosteroid guidelines
About a decade after the first corticosteroid treatment guidelines are published, AAN updates their
practice guidelines to address several key points:
Efficacy of corticosteroids for survival, quality of life, motor function, scoliosis, pulmonary
function, and cardiac function
Adverse events associated with corticosteroids
Interventions to maximize bone health
References
Gloss D, Moxley RT 3rd, Ashwal S, et al. Practice guideline update summary: Corticosteroid
treatment of Duchenne muscular dystrophy: Report of the Guideline Development Subcommittee of the
American Academy of Neurology. Neurology. 2016;86(5):465-472.
2017
Corticosteroid treatment approval
The first and only corticosteroid treatment for patients with DMD who are aged ≥5 years is approved in the United States by the FDA.
Slope of change in 6MWD from baseline to end of treatment is published as an alternate efficacy end
point in trials for DMD and may more accurately estimate the rate of change in 6MWD than previously
used methods.
This analysis accounts for the time to loss of ambulation, which is not accounted for in analyses of
change from baseline
References
Riebling P, Souza M, Elfring GL, et al. Slope analysis of 6-minute walk distance as an alternative
method to determine treatment effect in trials in Duchenne muscular dystrophy [abstract].
Eur J Paediatr Neurol. 2017;21(suppl 1):E94.
2018
Updated DMD guidelines
The updated DMD Care Considerations Guidelines are published in a 3-part series that includes:
Three new topics for discussion: primary care and emergency management, endocrine management,
and transitions of care across the life span of a patient with DMD
Dystrophin restorative therapies (e.g., ataluren and eteplirsen) as emerging treatments for DMD
Behavioral considerations for patients who are living longer owing to better disease management
options. Specifically, referral to a psychologist and/or speech-language pathologist is
appropriate when patients exhibit intellectual disability, attention deficit hyperactivity
disorder, or autism spectrum disorder
References
Birnkrant DJ, Bushby K, Bann CM, et al; DMD Care Considerations Working Group. Diagnosis and
management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular,
rehabilitation, endocrine, and gastrointestinal and nutritional management.
Lancet Neurol. 2018;17(3):251-267.
Colvin MK, Poysky J, Kinnett K, et al. Psychosocial management of the patient with Duchenne
muscular dystrophy.
Pediatrics. 2018;142 (suppl 2): S99-S109.
Updated DMD guidelines
The life expectancy of patients with DMD increases to 30 to 40 years of age; consequently, The DMD
Care Considerations Guidelines to diagnose and manage patients with DMD are updated to address the
evolving needs of older patients and potential disease-modifying therapies in development.
References
Birnkrant DJ, Bushby K, Bann CM, et al; DMD Care Considerations Working Group. Diagnosis and
management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation,
endocrine, and gastrointestinal and nutritional management.
Lancet Neurol. 2018;17(3):251-267.
Henricson EK, Abresch RT, Cnaan A, et al.; CINRG Investigators. The cooperative international
neuromuscular research group Duchenne natural history study: glucocorticoid treatment preserves
clinically meaningful functional milestones and reduces rate of disease progression as measured by
manual muscle testing and other commonly used clinical trial outcome measures.
Muscle Nerve. 2013;48(1):55-67.
Pandya S, James KA, Westfield C, et al. Health profile of a cohort of adults with Duchenne
muscular dystrophy. Muscle Nerve. 2018;58(2):219-223.
Name: Alan
Signs and symptoms at diagnosis
Gower’s maneuver, general muscle weakness, clumsiness, toe-walking, elevated creatine kinase
Age at diagnosis
4.5 years
Diagnostic method
Genetic sequencing for DMD,
which identified a nonsense mutation
Management/treatment options
Daily prednisone with dose adjustments as needed; management care team involvement (e.g.,
physical therapist, occupational therapist, speech-language pathologist, orthotist,
nutritionist)
Progression
Becomes non-ambulatory at 13 years of age;
no surgery needed for scoliosis
Outcome
Died at 32 years of age due to cardiac and respiratory complications
References
Birnkrant DJ, Bushby K, Bann CM, et al; DMD Care Considerations Working Group. Diagnosis
and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular,
rehabilitation, endocrine, and gastrointestinal and nutritional management.
Lancet Neurol. 2018;17(3):251-267.
Bushby K, Connor E. Clinical outcome measures for trials in Duchenne muscular dystrophy: report from International Working Group meetings. Clin Investig (Lond). 2011;1(9):1217-1235.
Ciafaloni E, Fox DJ, Pandya S, et al. Delayed diagnosis in Duchenne muscular dystrophy: data from the muscular dystrophy surveillance, tracking, and research network (MD STARnet). J Pediatr. 2009;155(3):380-385.
Pandya S, James KA, Westfield C, et al. Health profile of a cohort of adults with Duchenne
muscular dystrophy. Muscle Nerve. 2018;58(2):219-223.
Use of revised NSAA
The revised NSAA is employed as a clinical trial outcome measure to evaluate motor function according
to age-appropriate outcomes in young (2-5 years of age) patients with DMD that is caused by nonsense
mutations (nmDMD).
The FDA authorizes the first newborn screening test for DMD, which measures creatine kinase MM (CK-MM)
in dried blood spot samples, enabling diagnosis
before symptom onset.
Dr Tim Stenzel, director of the Office of In Vitro Diagnostics and Radiological Health in the
FDA’s Center for Devices and Radiological Health stated, “This authorization reflects our
commitment to fostering innovation in devices to help inform and provide options to patients and
their caregivers. Early screening can help identify individuals who need additional follow-up or
treatment.”
Expansion of indicated population for a corticosteroid treatment
The FDA expands the indicated population for an approved corticosteroid treatment to include patients with DMD aged 2 years of age and older, in line with clinical care guidelines supporting use of glucocorticoid treatment in the early ambulatory stage of the disease to slow disease progression.
References
Birnkrant DJ, Bushby K, Bann CM, et al; DMD Care Considerations Working Group. Diagnosis and
management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation,
endocrine, and gastrointestinal and nutritional management.
Lancet Neurol. 2018;17(3):251-267.
An expert panel of physicians who treat Duchenne and Becker muscular dystrophies come together to
provide guidance on treating people with muscular dystrophy during the COVID-19 pandemic.
References
Veerapandiyan A, Wagner KR, Apkon S, et al. The care of patients with Duchenne, Becker, and other
muscular dystrophies in the COVID-19 pandemic. Muscle Nerve. 2020;62(1):41-45.
Management during COVID-19
Some of this guidance to treat patients with muscular dystrophy during COVID-19 includes:
Ensure timely, uninterrupted care using telemedicine, single-provider or multidisciplinary
visits
Individual treatment decisions should be made between the multidisciplinary care team, and the
patient/family after considering the policies and precautions for COVID-19
Conduct clinical trials in accordance with institution and sponsor-specific policies and
implement site specific precautions for COVID-19 as required
References
Veerapandiyan A, Wagner KR, Apkon S, et al. The care of patients with Duchenne, Becker, and
other muscular dystrophies in the COVID-19 pandemic. Muscle Nerve. 2020;62(1):41-45.
2024+
Looking ahead
Over the years, the field has made many advances in the understanding of DMD and management of
patients with the disease. Ongoing and planned initiatives to further improve the lives of patients
with DMD include:
Increased awareness and availability of newborn screening tests (e.g., CK-MM) for DMD in the United
States and around the world to allow for timely diagnosis and improved preservation of motor
function through available treatments.
References
Birnkrant DJ, Bushby K, Bann CM, et al; DMD Care Considerations Working Group. Diagnosis and
management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation,
endocrine, and gastrointestinal and nutritional management.
Lancet Neurol. 2018;17(3):251-267.
Mendell JR, Shilling C, Leslie ND, et al. Evidence-based path to newborn screening for Duchenne
muscular dystrophy. Ann Neurol. 2012; 71(3):304-313.
Identification and development of biomarkers to facilitate earlier detection of DMD and its impact
on multiple organ systems (e.g., cardiac function)
STRIVE continuation
In an effort to recognize and support the rare disease community, PTC’s STRIVE program continues to
award grants to nonprofit organizations that are serving patients with DMD.